Things are looking up in 2021! Multiple states have rapidly passed new DPC laws and the mountain west is leading the way this year.
The Primary Care Enhancement Act (SB 128) has bipartisan support at the federal level. This deserves broad support. The language is the same as in prior years and would resolve any HSA debate for most DPC practices.
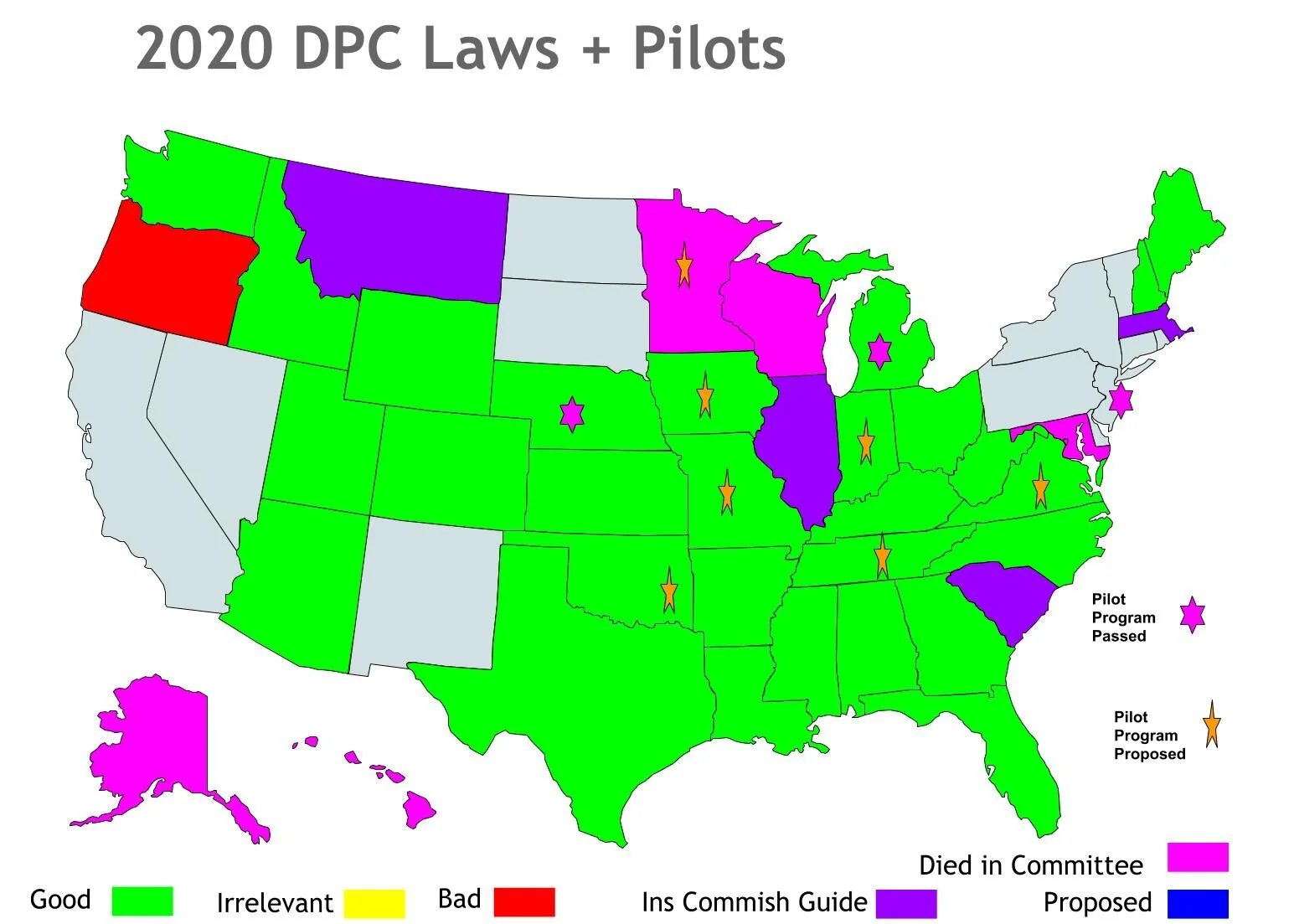
State Legislative Summary:
South Dakota is off to a great start this year with HB 1131. This bill is well drafted and deserves everyone’s full support. The legislative summary here shows that HB 1131 passed the House on 02/24/21 with a vote of 63-2. It passed the Senate 35-0 on 03/08/21 and it was signed by the Governor on 03/29/21 making South Dakota the 30th state to pass DPC defining “not insurance” legislation.
Montana - 2021 is a great year to be a DPC physician in Montana! This year SB 101 was passed to ensure that DPC is defined as outside of insurance in Montana. Montana had passed DPC not insurance legislation out of the house and senate on two prior occasions, but both were ultimately vetoed by the prior governor. Thankfully a wiser governor was in the office this time around and Montana became the 31st state to pass DPC defining “not insurance” legislation with his signature on 04/20/21. Less than one month later 05/11/21 Montana passed legislation permitting in-office dispensing.
Thanks to the efforts of Institute for Justice Attorney Josh Windham and Dr. Carol Bridges, Dr. Cara Harrop and Dr. Todd Bergland in May 2021 (in response to litigation from this group) the state passed SB 374 allowing healthcare providers in Montana to dispense medications directly to their patients. I have quoted some of the most important passages below and bolded a few areas of emphasis.
Now “a medical practitioner may dispense drugs if the practitioner:
(a) registers with the board of pharmacy provided for in 2-15-1733; and
(b) complies with the requirements of this section.
(2) Drugs dispensed by a medical practitioner must be:
(a) dispensed directly by the practitioner at the practitioner's office or place of practice;
(b) dispensed only to the practitioner's own patients; and
(c) necessary in the treatment of the condition for which the practitioner is attending the patient.
(3) Before dispensing a drug, a medical practitioner shall offer to give a patient the prescription in a written, electronic, or facsimile form that the patient may choose to have filled by the practitioner or any pharmacy.
(4) Except as otherwise provided in this section, a medical practitioner:
(a) may dispense only those drugs that the practitioner is allowed to prescribe under the practitioner's scope of practice; and
(b) may not dispense a controlled substance.
(5) A medical practitioner dispensing drugs shall comply with and is subject to the provisions of this part and the provisions of:
(a) Title 37, chapter 7, parts 4, 5, and 15;
(b) Title 50, chapter 31, parts 3 and 5;
(c) the labeling, storage, inspection, and recordkeeping requirements established by the board of pharmacy; and
(d) all applicable federal laws and regulations.
(6) A medical practitioner registering with the board of pharmacy shall pay a fee established by the board by rule. The fee must be paid at the time of registration and on each renewal of the practitioner's license.
(7) Except as provided in subsection (8), a medical practitioner registered with the board of pharmacy may not dispense drugs to an injured worker being treated pursuant to Title 39, chapter 71.
Subject only to 37-2-104, 37-7-401, and 37-7-402, this chapter does not: (1) subject a medical practitioner, as defined in 37-2-101, or a person who is licensed in this state to practice veterinary medicine to inspection by the board, prevent the person from compounding or using drugs, medicines, chemicals, or poisons in the person's practice, or prevent a medical practitioner from furnishing to a patient drugs, medicines, chemicals, or poisons that the person considers proper in the treatment of the patient.”
Prior to these updates in 2021 the Montana Code Annotated (2017) 37-2-104 historically stated that “it is unlawful for a medical practitioner to engage, directly or indirectly, in the dispensing of drugs” except… in an emergency, or “whenever there is no community pharmacy available to the patient,” or “the dispensing of drugs occasionally, but not as a usual course of doing business, by a medical practitioner.”
South Carolina is making efforts again with House Bill 4169. It was introduced and referred to committee on 04/07/21. The excellent and concisely written piece of DPC defining “not insurance” legislation deserves everyone’s full support. This is the language of the entire proposed law (also linked here).
Be it enacted by the General Assembly of the State of South Carolina:
SECTION 1. Chapter 61, Title 38 of the 1976 Code is amended by adding:
"Section 38-61-80.
(A) A direct primary care agreement is not a contract of insurance in this State and is not subject to regulation by the Department of Insurance.
(B) For the purposes of this section, a 'direct primary care agreement' means a written agreement between a patient or their legal representative and a health care provider that:
(1) allows either party to terminate the agreement in writing, without penalty or payment of a termination fee, at any time or after a notice period specified in the agreement not to exceed sixty days;
(2) describes the health care services to be provided in exchange for payment of a periodic fee;
(3) specifies the amount of the periodic fee and any additional fees to be paid by a third party;
(4) allows the periodic fee and any additional fees to be paid by a third party;
(5) prohibits the provider from charging or receiving additional compensation for health care services included in the periodic fee; and
(6) conspicuously and prominently states that the agreement is not health insurance and does not meet any individual health insurance mandate required by federal law."
Texas has revived legislation aimed at legalizing in office dispensing across the state with HB 1778. It was referred to committee on 03/10/21 and does not appear to be receiving much attention. The constitutional argument made by the Institute of Justice is now at the appellate stage. We should all be thankful for the efforts of Drs. Michael Garrett and Kris Held and attorneys Joshua Windham and Wesley Hottot.
Massachusetts is making an effort to allow physicians to dispense in their state as well. House Bill 2235 was referred to the Joint Committee on Public Health on 03/29/21. It is a simple and straightforward read. This is the entire bill:
“SECTION 1: Section 9 of Chapter 94C of the General Laws is hereby amended by striking out subsection (b), as so appearing, and inserting in place thereof the following:
(b) Notwithstanding section 17, a practitioner registered under section 7 may, in the good faith exercise of the practitioner’s clinical judgment, dispense by delivering to an ultimate user:
(1) Any prescription medication not regulated under this chapter;
(2) Any prescription medication classified by the department as schedule VI subject to such regulations as to safe storage, labeling, and recordkeeping as the department may adopt;
(3) Any prescription medication classified by the department as schedule II–V subject to such regulations as to safe storage, labeling, recordkeeping, dosage, and quantity as the department may adopt.
Before dispensing a prescription medication under this section, a practitioner must inform the ultimate user of their right to purchase the medication from any other practitioner registered under section 7. This section shall not be construed to restrict a practitioner from dispensing any prescription medication necessary to respond to a medical emergency.”
Maryland is rumored to be reviving their “not insurance” DPC legislative efforts this year as well (more details to come).
Discussions have supposedly been held in Alaska and Pennsylvania as well.
The Iowa Senate has passed a short (vague) piece of legislation proposing a Medicaid DPC pilot. It’s nice to have attention, but the devil is in the details. This bill has very little detail. The state is paying the bill rather than using the voucher system proposed in Oklahoma. This is not ideal. This is the entire text of the half page piece of legislation:
Section 1. DIRECT PRIMARY CARE AGREEMENTS——MEDICAID MEMBERS——PILOT PROGRAM. The department of human services shall develop and oversee a pilot program beginning January 31, 2022, and ending December 31, 2023, to allow Medicaid members in specified categories to receive primary care health services, as defined in section 135 N.1, through a direct primary care arrangement, with the Iowa Medicaid enterprise acting as the third-party payor for such services utilizing state only funds. The eligible Medicaid member categories shall include childless adults and pregnant women.
EXPLANATION The inclusion of this explanation does not constitute agreement with the explanation’s substance by the members of the general assembly. This bill requires the department of human services to develop and oversee a pilot program beginning January 1, 2022, and ending December 31, 2023, to allow Medicaid members in specified categories to receive primary care health services through a direct primary care arrangement, with the Iowa Medicaid enterprise acting as the third-party payor for such services utilizing state-only funds. The eligible Medicaid member categories shall include childless adults and pregnant women.
Other News:
Thank you to Dr. Maryal Concepcion for inviting me to be a part of her My DPC Story podcast!
Jeff and Frank launched TaroHealth last month to help patients learn about DPC, then find and join a nearby practice. They are increasing community awareness of the DPC model by creating a consumer-first, Airbnb-like experience designed specifically for patients. Taro is currently only available in Massachusetts, Connecticut, Virginia, and DC.
Dr. Doug Farrago has been doing a great job with entertaining and timely content over at DPC News. Check it out!
While it does not directly affect most DPC practices, some states (such as Arizona) are debating following Missouri’s lead and establishing an “assistant physician” category whereby medical school graduates without a residency can use their medical degree under the supervision of a fully licensed physician. Jeremy Snavely wrote an excellent overview here. Montana